May 21, 2026 | Body Contouring, Facelift
Preservation, Not Minimalism: How Modern Plastic Surgery Rethought Volume
A patient sat down in my consultation room last week, opened her phone, and showed me two photos.
The first was a friend of hers who had a breast augmentation in the early 2000s. The implants had drifted laterally over the years, and the breast tissue around them looked hollow on top. The second photo was a woman she had seen on Instagram from a recent operation. Smaller implants, fuller upper pole, a shape that read as natural. “I want what is in this second photo,” she told me, “but I am scared of what happens in twenty years.”
That conversation, almost exactly that conversation, is the reason I wrote my bylined manifesto for Connectively this month. The piece argues something patients keep hearing wrong. Modern plastic surgery is not going smaller. It is going from “addition at all costs” to “addition without collateral damage.” For most patients evaluating a procedure in 2026, that distinction will change the way you choose a surgeon.
This post walks through what the preservation shift actually means, in plain English, for the three procedure families where it matters most: breast augmentation, gluteal fat grafting, and facial volume restoration.
What “Preservation” Actually Means In Plain English
The word gets used a lot now. So I want to define it carefully, because most patients hear “preservation” and assume “minimalism.” Those are two different ideas.
Preservation, as the field uses the word, is a planning framework. The surgeon decides first what tissue or anatomy must be left intact, and then plans the operation around that constraint. That is the order of operations. Anatomy first, volume second. Twenty years ago we did it the other way around: volume goal first, with the anatomy paying whatever cost the volume required.
In practice, preservation means three things in my operating room.
First, ligament-sparing dissection. When I open a pocket for a breast implant or undermine the deep plane of a face, I respect the suspensory ligaments and retaining ligaments wherever I can. Those ligaments are what keep tissue in position years after the surgery is done. If I cut them, I am putting that patient on a slow-motion collision course with bottoming out, malposition, or a second operation.
Second, plane-respecting technique. Every body part has anatomic planes (predictable layers of fascia, fat, and muscle). Modern technique stays in the right plane. Modern technique also uses imaging (ultrasound, in the case of fat grafting) to confirm the plane in real time. That is not technology for technology’s sake. That is patient safety made visible.
Third, compartment-specific volume restoration. Especially in the face. Patients who have lost facial volume to aging have lost it in specific deep compartments. Restoring volume to the wrong compartment, even a small amount, looks unnatural. Restoring it to the right compartment, even a generous amount, looks like a younger version of the same face. The skill is anatomic literacy.
A patient does not need to memorize any of that to evaluate a surgeon. A patient needs to know that those three ideas exist, and that a surgeon worth choosing will be able to talk about them.
What Preservation Looks Like In My Practice
I want to walk through the three procedure families one at a time, because the trade-offs in each one are different.
Breast Augmentation
For thirty years, the standard breast augmentation involved a wide pocket dissection. The implant looked great in the early years. The breast tissue and the ligaments that hold the breast up against gravity were, frankly, not the focus.
What I do today is different.
I use ergonomic implants, primarily the Motiva line, which are lighter for their volume and shaped to move with the breast tissue rather than sit as a rigid shell behind it. That alone reduces the long-term load on the soft tissue scaffold. I dissect a more precise pocket, narrower in the right places, with the inframammary ligament along the breast fold preserved. The patient leaves with a result that looks finished on day one. The five-year and ten-year shape is what tells me whether the case was actually done right.
If you want a deeper read on this specifically, see my Motiva Preserve case study on this site. That post walks through a 315 cc athletic-build patient who was back in the gym at two weeks because the soft-tissue trauma was so much lower than a wide-pocket dissection would have required.
Gluteal Fat Grafting (BBL)
This is the procedure that has had the biggest safety transformation of any procedure in the field in the last fifteen years. Not because we lowered volumes (we did not), but because we changed the plane.
Twenty years ago, BBL technique grafted into and sometimes through the gluteal fascia, into deeper planes that we now know are unsafe. The risk was fat embolism. A subset of patients did not survive it. That is not a minor footnote. That is the entire reason ultrasound guidance is now considered the standard of care for high-volume gluteal fat grafting.
In my OR, every BBL is ultrasound-guided. The ultrasound probe sits on the buttock during cannulation. I see the fascia. I see the cannula. I see, in real time, whether I am in the safe subcutaneous plane. That is preservation: I am preserving the patient from a complication that older technique could not see and therefore could not avoid.
Volumes have not collapsed. In well-selected patients with adequate donor sites, I will graft three hundred to five hundred cc per side safely. The volume is not the safety story. The plane is the safety story.
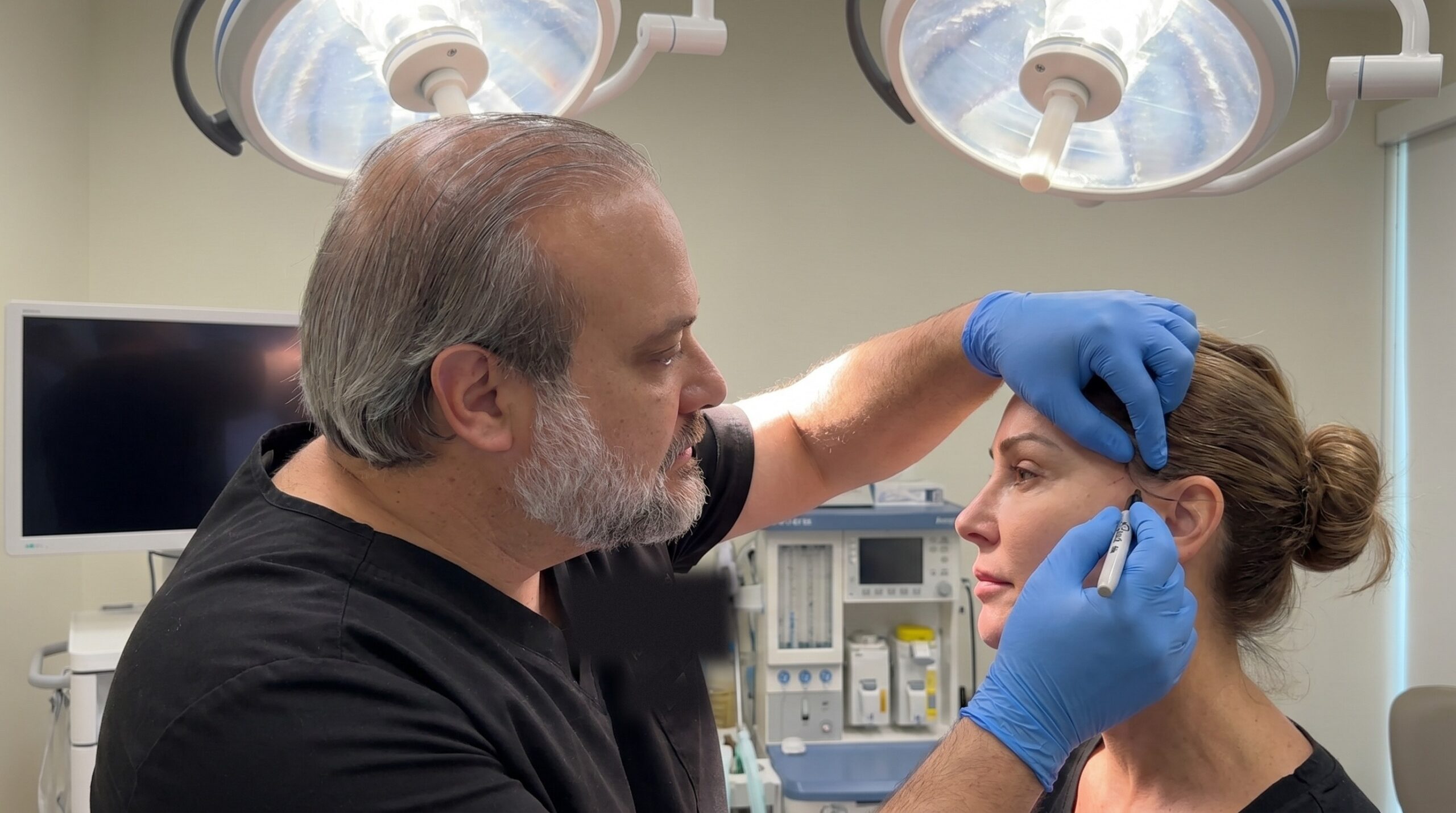
Facial Volume
This is the most counterintuitive piece for patients, so I want to flag it directly.
A preservationist surgeon will, on most facelift and midface patients today, restore more facial volume than a surgeon following the playbook from ten years ago. Not less. More.
The reason is the data. Long-term volumetric studies of facial aging have made it clear how much volume the face loses over decades, especially in the deep fat compartments and along the bony architecture. When we ignore that loss and try to fix an aging face by tightening skin, we produce the pulled, lateralized look patients dread. When we replace the lost deep volume in the correct compartments, the patient looks like a younger version of themselves rather than a tighter version.
In my facelift cases, I am routinely placing autologous fat into the deep medial cheek, the buccal extension, and along the pyriform aperture. I am using endoscopic access (the Ponytail Lift approach for the midface) to reposition the facial fat pads at their native deep plane. The skin envelope does less work because the architecture underneath is back where it belongs. That is what produces the “you look rested, did you sleep more?” reaction at six months and the “you do not look operated on” reaction at ten years.
How To Evaluate A Surgeon’s Approach Before You Book
Patients ask me, sometimes apologetically, how they should compare surgeons during the consult phase. There is no need to apologize. These are good questions and you should be asking them.
For a breast augmentation consult, ask the surgeon:
- How wide is your pocket dissection, and how do you decide?
- How do you handle the inframammary ligament?
- Are you using ergonomic implants or traditional shells?
- What does the breast typically look like at year five and year ten in your hands?
For a gluteal fat grafting consult, ask:
- Do you use intraoperative ultrasound guidance? On every case?
- Which plane do you graft into?
- What total volume per side do you graft, and what determines your upper limit for me?
For a facelift or facial volume consult, ask:
- What facial compartments are you targeting on me?
- At what depth are you placing volume?
- What is your approach for the deep medial cheek, the buccal extension, and the pyriform?
A surgeon comfortable with these questions can answer them in patient-friendly language without sounding rehearsed. A surgeon who answers only with total volume numbers, with no thought to plane, ligament, or compartment, is operating from an older playbook. That is the signal.
If you want to bring this article to a consultation with another surgeon, take a screenshot of this section. Use it as your question list. Any surgeon worth the consult fee will appreciate that you came prepared.
Why I Approach Surgery This Way
My training has been on both sides of this transition.
I completed my plastic surgery fellowship at the Mayo Clinic and was board-certified in plastic surgery (2010) after general-surgery certification (2008). My subsequent training in deep plane and Ponytail Lift facelift technique was done at the Ponytail Academy intermediate course in Pittsburgh and the advanced course in Santa Monica. I currently hold a Clinical Associate Professor of Plastic Surgery appointment at Texas Tech University Health Sciences Center Paul L. Foster School of Medicine, where I teach residents.
That teaching role keeps me honest. Residents ask the questions patients should ask. “Why are you cutting that ligament? Why are you grafting that volume into that plane? Why that compartment?” If the answer is “that is how I was taught,” that is not a good enough answer in 2026. Preservation is the framework that survives the question.
I have been recognized as a Castle Connolly Top Doctor for thirteen consecutive years (2014 through 2026), which I mention only because it indexes longitudinal patient outcomes more than press cycles. Long-term shape is what we are talking about here. That is the standard I want to be held to.
A Short FAQ
Does a “preservationist” surgeon do smaller procedures? Not necessarily. The implant volume, the graft volume, the facial volume can all be the same or higher than a generation ago. What changes is what the surgeon refuses to damage to deliver that volume.
Is preservation only for first-time surgery, or also for revisions? Both, but the calculation is different. In revision surgery, much of the preservable anatomy has already been altered. The framework then becomes: what is left, and how do we rebuild structure where prior surgery removed it.
What about fillers? Are they part of preservation? Fillers are a different conversation. Used correctly and in small amounts in specific compartments, they can be useful. Used as a substitute for compartment-specific deep volume restoration, they push patients into the overfilled, surface-level look most people are trying to avoid. I cover that in more detail in my drworldwide.com piece on the same Connectively manifesto.
Where can I read the full bylined Connectively article? At blog.connectively.us. It is a roughly four-minute read.
For an editorial version of this argument written in my own first-person voice, see my piece on drworldwide.com: Preservation, Not Minimalism: I Wrote a Manifesto for Connectively.
Ready To Schedule A Consultation?
Dr. Frank Agullo, MD, FACS, is a double board-certified plastic surgeon with a Mayo Clinic plastic surgery fellowship and advanced Ponytail Academy training (Pittsburgh and Santa Monica). To schedule a consultation at Agullo Plastic Surgery in El Paso, Texas, call (915) 590-7900 or text 1-866-814-0038. You can also book online at agulloplasticsurgery.com/appointments. Follow Dr. Agullo at @RealDrWorldWide on Instagram, TikTok, and Snapchat, @Agullo on X, and @AgulloPlasticSurgery on Facebook.
#StayBeautiful